3.6 Household Details
- Step 1: Citizenship information
- Step 2: People with a disability, illness, or injury
- Step 3: Hospitalization information
- Step 4: Your household’s health
- Step 5: Medicare coverage
- Step 6: Food assistance
- Step 7: FoodShare Basic Work Rules Information
- Step 8: FoodShare Work Requirement Information
- Step 9: Child care help
- Step 10: School enrollment
- Step 11: Legal history
- Step 12: Confirm Information on the Summary Page
Use these instructions to help people answer questions regarding people in the household. It can be started any time after the applicant has completed the Household Members section. The applicant may see different questions and pages, depending on which program or programs they selected. Once completed, the applicant can review the section for accuracy before going to the next section.
Step 1: Citizenship information
These pages ask the applicant for information about their citizenship status.
The “Citizenship information” page asks if there are any household members who aren't U.S. citizens.
Show/Hide an example of the pageShow/Hide an example of the page

| Questions | How to answer |
| Are all household members U.S. citizens? |
Select Yes or No. |
|
Who isn't a U.S. citizen?
|
Select the names of each household member who isn't a citizen of the U.S. |
If at least one person in the household isn't a U.S. citizen, the “_____’s immigration information” page displays.
This page asks about one household member at a time. It is repeated for each household member who isn't a U.S. citizen.
Show/Hide an example of the pageShow/Hide an example of the page

| Questions | How to answer |
| Does _____ have a sponsor? |
Select Yes or No. |
| Where was _____ born? (optional) | Select the country the person was born in from the dropdown menu. |
| When did _____ come to live in the U.S.? (optional) | Select the date from the calendar. |
| What is _____'s immigration status? (optional) | Select their immigration status from the dropdown menu. |
| When did _____ get this immigration status? (optional) | Select the date from the calendar. |
| What immigration card or document does _____ have? (optional) | Select their immigrant card or document from the dropdown menu. Their selection determines which of the document ID questions are asked. They only see the questions that match their ID type. |
|
What is _____’s Alien/USCIS number? (optional)
|
Enter their Alien/USCIS number. |
|
What is _____’s card number? (optional)
|
Enter their card number. |
|
What is _____’s employment authorization expiration date? (optional)
|
Select the date from the calendar. |
|
What is _____’s Certificate of Citizenship number? (optional)
|
Enter their Certificate of Citizenship number. |
|
What is _____’s Certificate of Naturalization number? (optional)
|
Enter their Certificate of Nationalization number. |
|
What is _____’s passport number? (optional)
|
Enter their passport number. |
|
What country is _____’s passport from (optional)
|
Select their passport’s issuing country from the dropdown menu. |
|
What is _____’s I-94 number? (optional)
|
Enter their I-94 number. |
|
What is _____’s passport expiration date? (optional)
|
Select the date from the calendar. This is found on the identification page of the passport. |
|
What is _____’s SEVIS ID? (optional)
|
Enter their SEVIS ID number. |
|
Please describe _____’s immigration card or other document. (optional)
|
Enter a description of the document. |
| Does _____ meet military service requirements? (optional) | Select Yes, No, or I don’t know. |
Katie Beckett Medicaid-only applications answer separate citizenship questions for just those applying for Katie Beckett Medicaid. Citizenship status is only considered for other household members when additional benefit programs are also requested for the household.
Show/Hide an example of the pageShow/Hide an example of the page
.png)
| Questions | How to answer |
| Are all household members U.S. citizens? |
Select Yes or No. If the applicant selects no, the next question displays |
|
Who isn't a citizen?
|
Select the names of each household member who isn't a citizen of the U.S. |
For Katie Beckett Medicaid-only applications with applicants without U.S. citizenship, the following optional questions display.
Show/Hide an example of the pageShow/Hide an example of the page
.png)
Step 2: People with a disability, illness, or injury
These pages ask for information about the household’s disability determination.
The pages that display vary based on which programs or combination of programs the applicant is requesting.
The People with a disability, illness, or injury page asks applicants with a health care and/or FoodShare request if any household members are blind, disabled, or can’t work because they are ill or injured. These people may have more benefit options or different program requirements.
Show/Hide an example of the pageShow/Hide an example of the page

| Questions | How to answer |
| Is anyone in your household blind, living with a disability, or unable to work because of an illness or injury? |
Select Yes or No. |
|
Who is blind, living with a disability, or unable to work because of an illness or injury?
|
Select which member or members of the household is blind, has a disability or has an illness. |
If the applicant selects yes, the More about _____’s disability, illness, or injury page displays.
This page asks about the people identified as blind or disabled and repeats for all household members who were identified as blind or disabled on the previous page.
Show/Hide an example of the pageShow/Hide an example of the page

| Questions | How to answer |
| Has the Social Security Administration officially determined that _____ is blind? |
Select Yes, No, or Waiting for a decision. |
| Has the Social Security Administration officially determined that _____ has a disability? | Select Yes, No, or Waiting for a decision. |
|
Will _____ submit a Medicaid Disability Application (MADA) within the next 30 days to get an official decision about _____’s blindness or disability?
|
This question only displays if the applicant selected no on one or both of the previous the questions. Select Yes or No. The MADA must be completed and approved in order to be considered blind or disabled for program policy. |
| Does _____ have work expenses related to their blindness or disability? (optional) | Select Yes, No, or I don’t know. |
| Is _____ unable to work because of an illness or injury? (optional) | Select Yes, No, or I don’t know. |
Alternatively, the People with a disability page asks applicants with a Katie Beckett Medicaid-only request, or a Katie Beckett Medicaid request combined with Wisconsin Shares Child Care, Family Planning Only Services, JAL, EA, or Wisconsin Works (W-2), if any household members are disabled.
Show/Hide an example of the pageShow/Hide an example of the page
.png)
| Questions | How to answer |
|
Are any of these household members living with a disability? *[First Name, Last Name] *[First Name, Last Name] |
Select Yes or No. Don't include someone who can't work because of pregnancy. If the applicant selects yes, the next questions displays. |
|
Who is living with a disability?
|
Select which of the household members listed has a disability. |
If the applicant selects yes, the More about _____'s disability page displays.
This page asks about the people identified as blind or disabled and repeats for all household members who were identified as disabled on the previous page.
Show/Hide an example of the pageShow/Hide an example of the page
.png)
| Questions | How to answer |
| Has the Social Security Administration officially determined that _____ has a disability? | Select Yes, No, or Waiting for a decision. |
|
Will _____ submit a Medicaid Disability Application within the next 30 days to get an official decision about _____'s disability?
|
This questions only displays if the applicant selected no on the previous question. Select Yes or No. If the Medicaid Disability Application isn't completed, Katie Beckett Medicaid-only applicants are required to go through a separate disability determination process. |
The next page the applicant sees depends on which programs the applicant is applying for.
| If the application includes: | Continue to: |
| Katie Beckett Medicaid | Step 3: Hospitalization information |
| All other programs | Step 4: Your household's health |
Step 3: Hospitalization information
This page asks for hospitalization information for Katie Beckett Medicaid household members.
Show/Hide an example of the pageShow/Hide an example of the page
.png)
| Questions | How to answer |
|
Were any of these household members hospitalized in the past three months? *[First Name, Last Name] *[First Name, Last Name] |
Select Yes or No. If the applicant selects yes, the next question displays. |
|
Who was hospitalized in the past three months?
|
Select which member of the household was hospitalized in the past three months. |
If the applicant selects yes, the More about ____'s hospitalization page displays.
This page asks about the person(s) identified as hospitalized and repeats for all household members who were identified as hospitalized on the previous page.
Show/Hide an example of the pageShow/Hide an example of the page
.png)
| Questions | How to answer |
| When was [First Name] admitted into a hospital? (optional) | Enter the date that the person was admitted into the hospital. |
| When was [First Name] discharged from a hospital? (optional) | Enter the date that the person was discharged from the hospital. |
Step 4: Your household’s health
This page asks about health situations that household members may be experiencing.
Show/Hide an example of the pageShow/Hide an example of the page

| Questions | How to answer |
| Does anyone in your household need help with activities of daily living? | Select Yes or No. If the applicant selects yes, the next question displays. |
|
Who needs help?
|
Select which member or members of the household needs help. |
| Has anyone in your household been diagnosed with tuberculosis? | Select Yes or No. If the applicant selects yes, the next question displays. |
|
Who has been diagnosed tuberculosis?
|
Select which member or members of the household has tuberculosis. |
| Has anyone in your household been in an accident in the last three months? | Select Yes or No.
By accidents, we mean:
If the applicant selects yes, the next question displays. |
|
Who was in an accident?
|
Select the member or members of the household that was in an accident. |
| Has anyone in your household had a medical emergency in the last three months? | Select Yes or No. By medical emergency, we mean a medical problem that could put a household member's health at serious risk if they don't get medical care right away. This doesn't include ongoing or chronic conditions. If the applicant selects yes, the next question displays. |
|
Who had a medical emergency?
|
Select the member or members of the household that recently had a medical emergency. |
If no household member lives in a care facility, go to the table below to see which step to complete next.
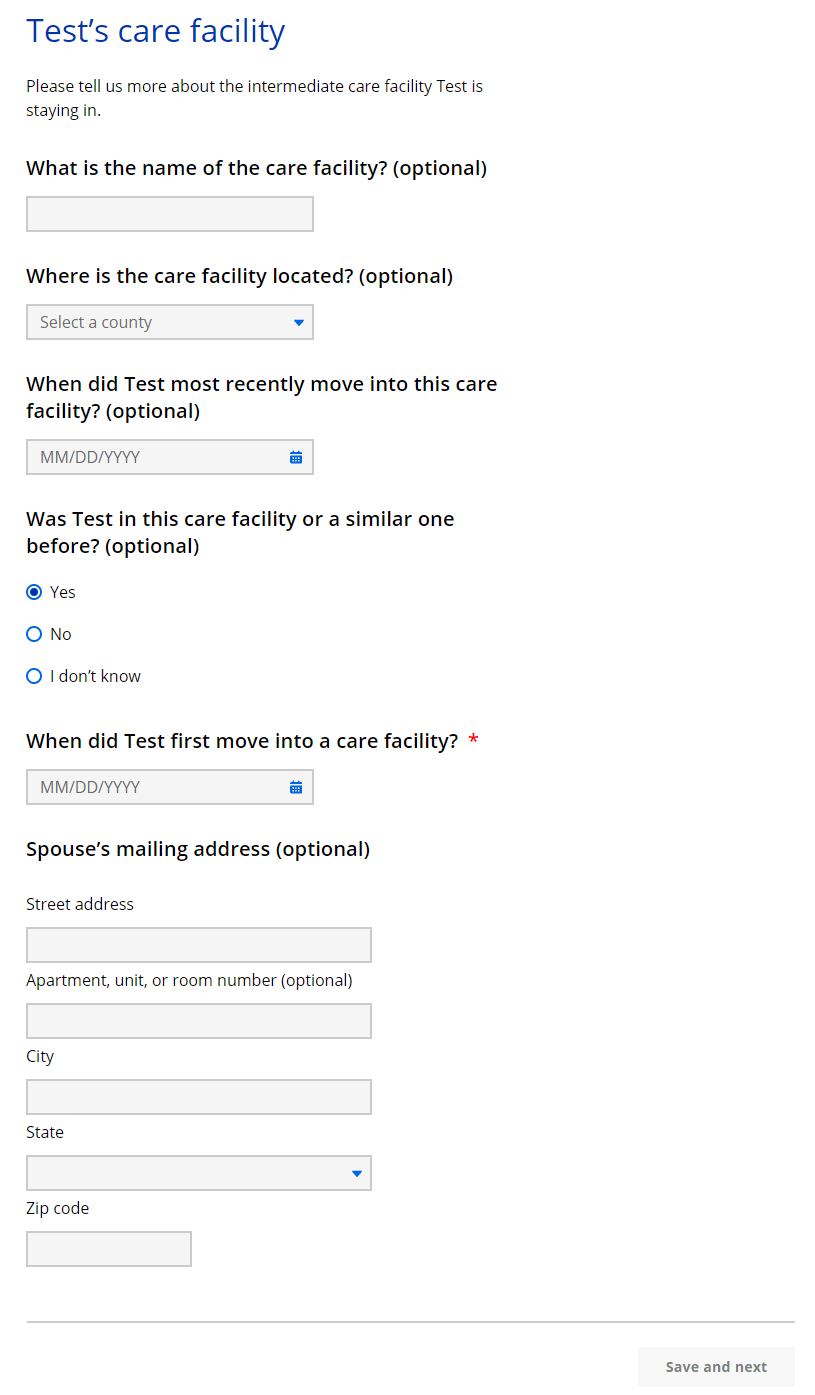
If at least one adult in the household is currently living in a care facility, the _____’s care facility page displays.
Show/Hide an example of the pageShow/Hide an example of the page
The next page the applicant sees depends on which programs the applicant is applying for.
| If the application includes... | Continue to... |
| FoodShare, health care, or Family Planning Only Services | Step 5: Medicare coverage |
| Wisconsin Shares Child Care Subsidy and does not include FoodShare, health care, or Family Planning Only Services | Step 9: Child care help |
| Only W-2 or JAL | Step 10: School enrollment |
Step 5: Medicare coverage
The Medicare coverage page only displays if the application includes FoodShare, health care, or Family Planning Only Services and asks if there are any household members receiving Medicare Part A or Part B.
Show/Hide an example of the pageShow/Hide an example of the page
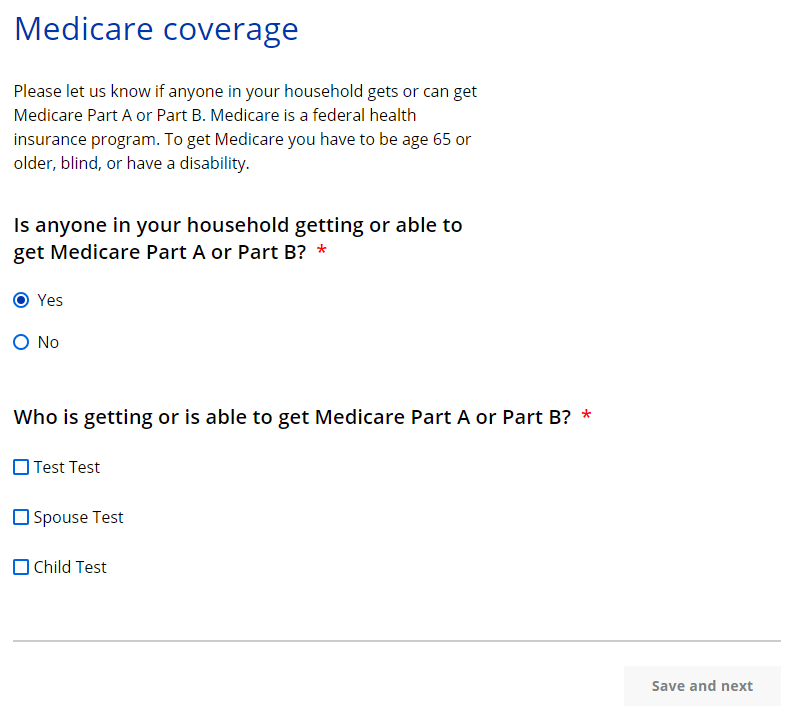
| Questions | How to answer |
| Is anyone in your household getting or able to get Medicare Part A or Part B? |
Select Yes or No. |
|
Who is getting or is able to get Medicare Part A or Part B?
|
Select which member or members of the household that is in the process of getting or is eligible to get Medicare. |
If the applicant selects yes, the _____’s Medicare coverage page displays.
This page asks about the Medicare coverage of household members receiving Medicare Part A or B and repeats for all household members who are receiving or eligible for Medicare Part A or B.
Show/Hide an example of the pageShow/Hide an example of the page
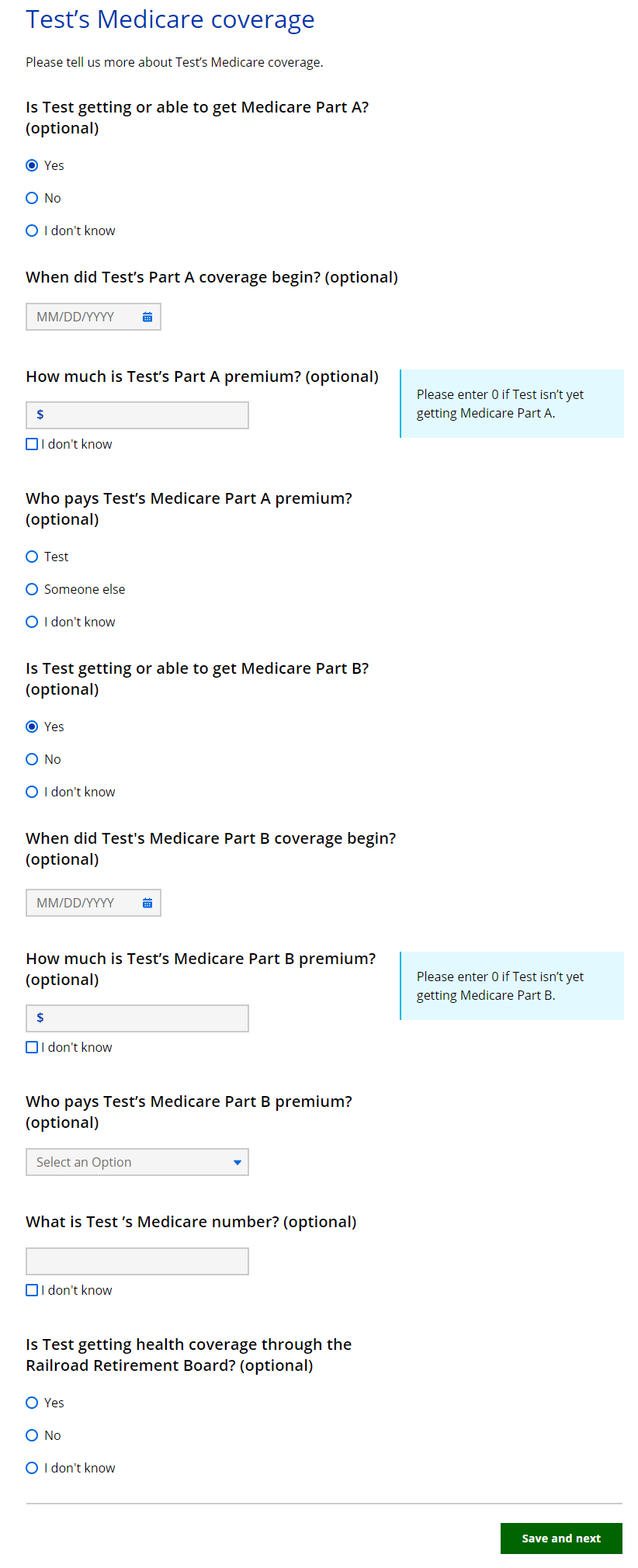
| Questions | How to answer |
| Is _____ getting or able to get Medicare Part A? (optional) |
Select Yes, No, or I don’t know. If the applicant selects yes, the next three questions display. |
|
When did _____’s Part A coverage begin? (optional)
|
Select date from the calendar. |
|
How much is _____’s Part A premium? (optional)
|
Enter the premium. Enter “0” if applicant is not yet receiving Medicare Part A. The applicant may also select I don’t know instead of entering a number. |
|
Who pays _____’s Medicare Part A premium? (optional)
|
Select Me, Someone else, or I don’t know. |
| Is _____ getting or able to get Medicare Part B? (optional) |
Select Yes, No, or I don’t know. If the applicant selects yes, the next three questions display. |
|
When did _____’s Medicare Part B coverage begin? (optional)
|
Select date from the calendar. |
|
How much is _____’s Medicare Part B premium? (optional)
|
Enter the premium. Enter “0” if applicant isn't yet receiving Medicare Part B. The applicant may also select I don’t know instead of entering a number. |
|
Who pays _____’s Medicare Part B premium? (optional)
|
Select Me, Someone else, or I don’t know. |
| What is _____’s Medicare number? (optional) | Enter Medicare number. The applicant may also select I don't know _____’s Medicare number instead of entering a number. |
| Are you getting health coverage through the Railroad Retirement Board? | Select Yes, No, or I don’t know. |
The next page the applicant sees depends on if the household includes a childless adult and which programs they are applying for.
A childless adult is an adult aged 19-64 who isn't pregnant and doesn't have dependent children living in the home.
| If the household includes... | And the application includes... | Continue to... |
| Someone older than 20 years old | W-2 or JAL only | Step 10: School enrollment |
| Neither of the above | FoodShare | |
| Wisconsin Shares Child Care Subsidy and not FoodShare | Step 9: Child care help | |
| Health care or FPOS only | Step 12: Confirm the information on the Summary page |
Step 6: Food assistance
This page only displays if the application includes FoodShare and asks about any SNAP Benefits or Tribal nation commodities being received and prior FSET sanctions.
Show/Hide an example of the pageShow/Hide an example of the page
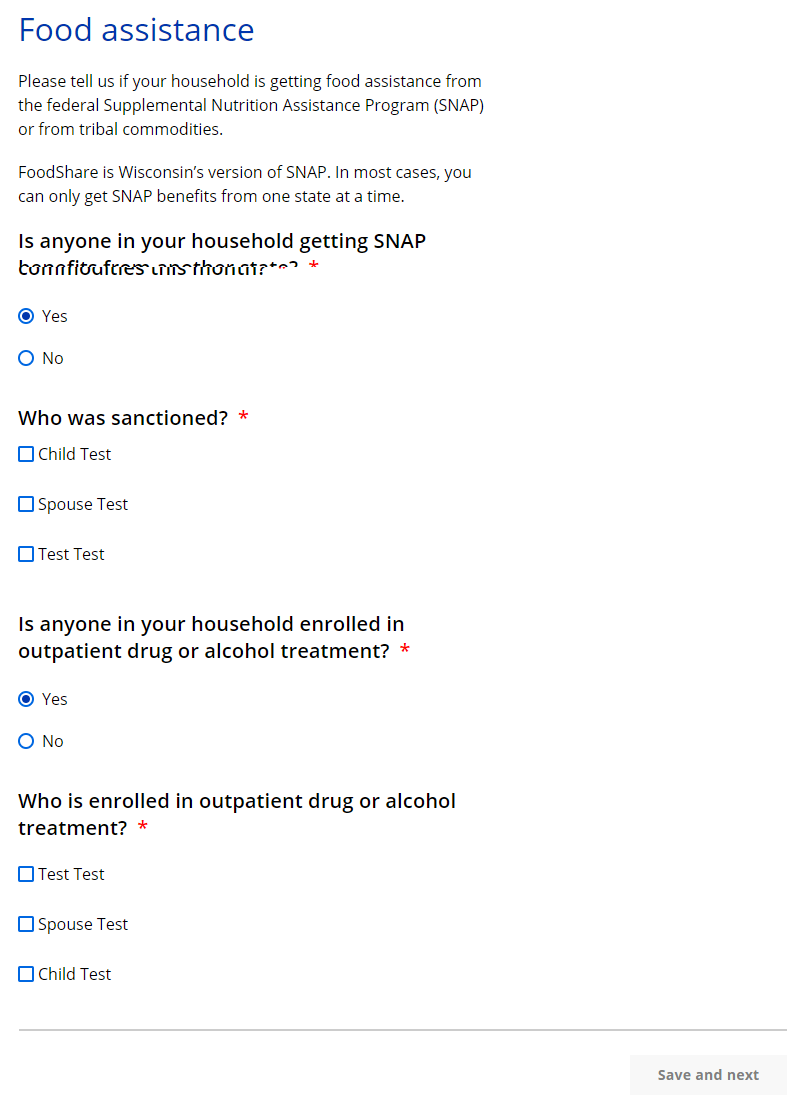
| Questions | How to answer |
| Is anyone in your household getting SNAP benefits that were sanctioned? |
Select Yes or No. If the applicant selects yes, the next question displays. |
|
Who was sanctioned?
|
Select which member or members of the household was sanctioned. |
| Is anyone in your household enrolled in outpatient drug or alcohol treatment? |
Select Yes or No. If the applicant selects yes, the next question displays. |
|
Who is enrolled in outpatient drug or alcohol treatment?
|
Select which member or members of the household are enrolled in outpatient drug or alcohol treatment. |
The next page the applicant sees depends on which programs the applicant is applying for.
| If the household includes... | And the application includes... | Continue to... |
| Someone between 16-59 years old | FoodShare | |
| Someone older than 20 years old | W-2 or JAL only | Step 10: School enrollment |
| No one older than 20 years old | Wisconsin Shares Child Care Subsidy | Step 9: Child care help |
| Any other programs | Step 10: School enrollment |
Step 7: FoodShare Basic Work Rules Information
The FoodShare Basic Work Rules Information page only displays if the application includes a:
- FoodShare request.
- Completed "Food assistance" page (Step 5).
- Household member or members aged 16-59.
This step includes questions to ask about possible exemptions from the FoodShare Basic Work Rules for applicable household members.
Show/Hide an example of the pageShow/Hide an example of the page
.png)
| Question | How to Answer |
| Is anyone in your household in a Wisconsin Works (W-2) work program? (optional) |
Select Yes or No. If the applicant selects no, move on to the next question. If the applicant selects yes, a new follow-up question displays below. |
|
Who is in a Wisconsin (W-2) program
|
Select which household member(s) is in compliance with W-2 work program. |
| Is there a household member caring for a child under age 6 who does not live with them? (optional) |
Select Yes or No. If the applicant selects no, go to the next question. If the applicant selects yes, a new follow-up question displays below. |
|
Who is responsible for caring for a child under age 6 who does not live with them?
|
Select which household member(s) is responsible for caring for a child under age 6 who does not live with them. |
| Is anyone in your household responsible for caring for another person who cannot care for themselves? (optional) |
Select Yes or No. If the applicant selects no, go to the next question. If the applicant selects yes, a new follow-up question displays below. |
|
Who is responsible for caring for another person who cannot care for themselves?
|
Select which household member(s) is responsible for caring for another person who cannot care for themselves. |
The next page displayed depends on which programs the applicant is applying for.
| If the household includes... | And the application includes... | Continue to... |
| Someone between 18-54 years old | FoodShare | Step 8: FoodShare Work Requirement Information |
| Someone older than 20 years old | W-2 or JAL only | Step 10: School Enrollment |
| No one older than 20 years old | Wisconsin Shares Child Care Subsidy | Step 9: Child Care Help |
| Any other programs | Step 10: School Enrollment |
Step 8: FoodShare Work Requirement Information
The FoodShare Work Requirement Information page only displays if the application includes a:
- FoodShare request.
- Completed "Food assistance" page (Step 5).
- Completed "FoodShare basic work rules information" page (Step 6).
- Household member or members aged 16-59.
This step includes questions to ask about possible exemptions from the FoodShare work requirement for applicable household members.
Show/Hide an example of the pageShow/Hide an example of the page
.png)
| Questions | How to answer |
| Is anyone in your household a veteran? (optional) |
Select Yes or No. If the applicant selects no, go to the next question. If the applicant selects yes, a new follow-up question displays below. |
|
Which household member is a veteran?
|
Select which household member is a veteran of the United States Armed Forces who has been discharged or released under any condition. |
| Is anyone in your household an 18 to 24-year-old who was in foster care, a subsidized guardianship, or court-ordered kinship care when they turned 18? (optional) |
This questions displays when there is a household member listed as between age 18-24 years old. Select Yes or No. If the applicant selects no, go to the next question. If the applicant selects yes, a new follow-up question displays below. |
|
Who is an 18-24 year-old who was in foster care, subsidized guardianship, or court-ordered kinship care when they turned 18?
|
Select which household member is 18-24 years old and was in foster care, subsidized guardianship, or court-ordered kinship care when they turned 18. |
| Is anyone in your household participating in a work program? (optional) |
Select Yes or No. If the applicant selects no, go to the next question. If the applicant selects yes, a new follow-up question displays below. |
|
Who is participating in a work program?
|
Select which household member is participating in a work program. |
If no household member participates in a work program, go to the table below to see which step to complete next.
If at least one adult in the household is currently participating in a work program, the ____'s work program page displays with required questions about the work program.
The page is repeated depending on the number of household members participating in a work program.
Show/Hide an example of the pageShow/Hide an example of the page
.png)
| Question | How to answer |
| Which work program is ____ participating in? |
Select which type of work program the household member is participating in from one of the options in the drop-down menu:
|
| About how many hours per month does ____ participate in this program? |
Enter the number of hours the household member participates per month. Hours must be written as two-digit (up to 99). The page repeats for the other people selected. |
When the applicant completes Step 7: FoodShare Basic Work Rules Information and Step 8: FoodShare Work Requirement Information, they can view a PDF summary table with each question's response from the applicable pages.
Show/Hide an example of the pageShow/Hide an example of the page
.png)
.png)
The next page displayed depends on which programs the applicant is applying for.
| If the household includes: | And the application includes: | Continue to: |
| Someone older than 20 years old | W-2 or JAL only | Step 10: School enrollment |
| No one older than 20 years old | Wisconsin Shares Child Care Subsidy | Step 9: Child care help |
| Any other programs | Step 10: School enrollment |
Step 9: Child care help
This page only displays if the application includes Wisconsin Shares Child Care subsidy and asks if there are any household members engaged in any of the approved activities for the subsidy.
Show/Hide an example of the pageShow/Hide an example of the page

| Questions | How to answer |
| Does anyone in your household need help paying for child care while they work, go to school, or work and go to school? |
Select Yes or No. |
|
Who needs help paying for child care?
|
Select which member or members of the household need help paying for child care. |
The next page the applicant sees depends on which programs the applicant is applying for.
| If the household includes... | And the application includes... | Continue to... |
| Someone older than 20 years old | Wisconsin Shares Child Care Subsidy, W-2, or JAL only | Step 10: School enrollment |
| No one older than 20 years old | Any other programs | Step 11: Legal history |
Step 10: School enrollment
The School Enrollment page asks if there are any household members over 20 currently in school. This page only displays if the application includes Wisconsin Shares Child Care Subsidy, W-2, or JAL and all household members are outside of the age range where school enrollment information is required.
Show/Hide an example of the pageShow/Hide an example of the page
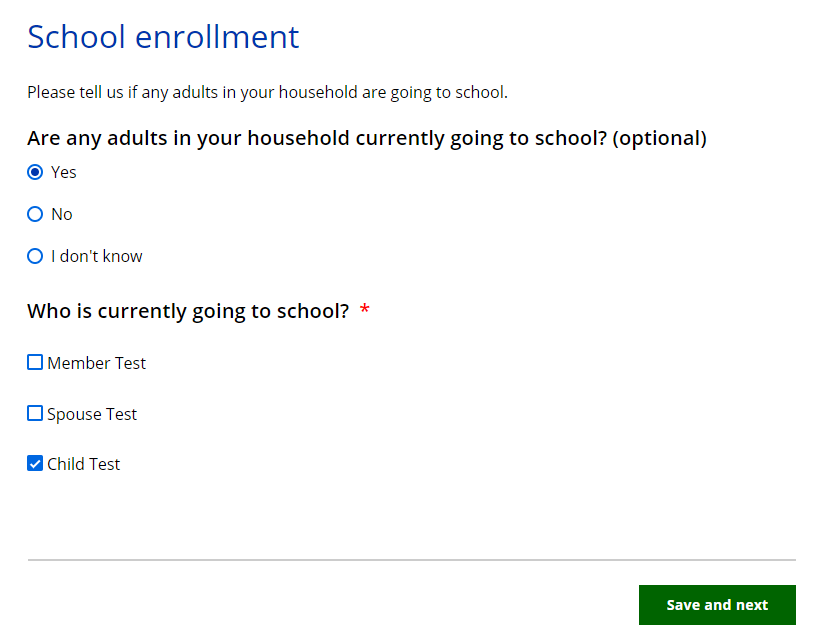
| Questions | How to answer |
| Are any adults in your household currently going to school? (optional) |
Select Yes, No, or I don’t know. |
|
Who is currently going to school?
|
Select which member or members of the household that are currently enrolled in school. |
If anyone in the household needs to provide school details based on the previous page, the _____’s education page displays. This page asks about school enrollment information for all individuals who fall into a required range for each program.
Show/Hide an example of the pageShow/Hide an example of the page
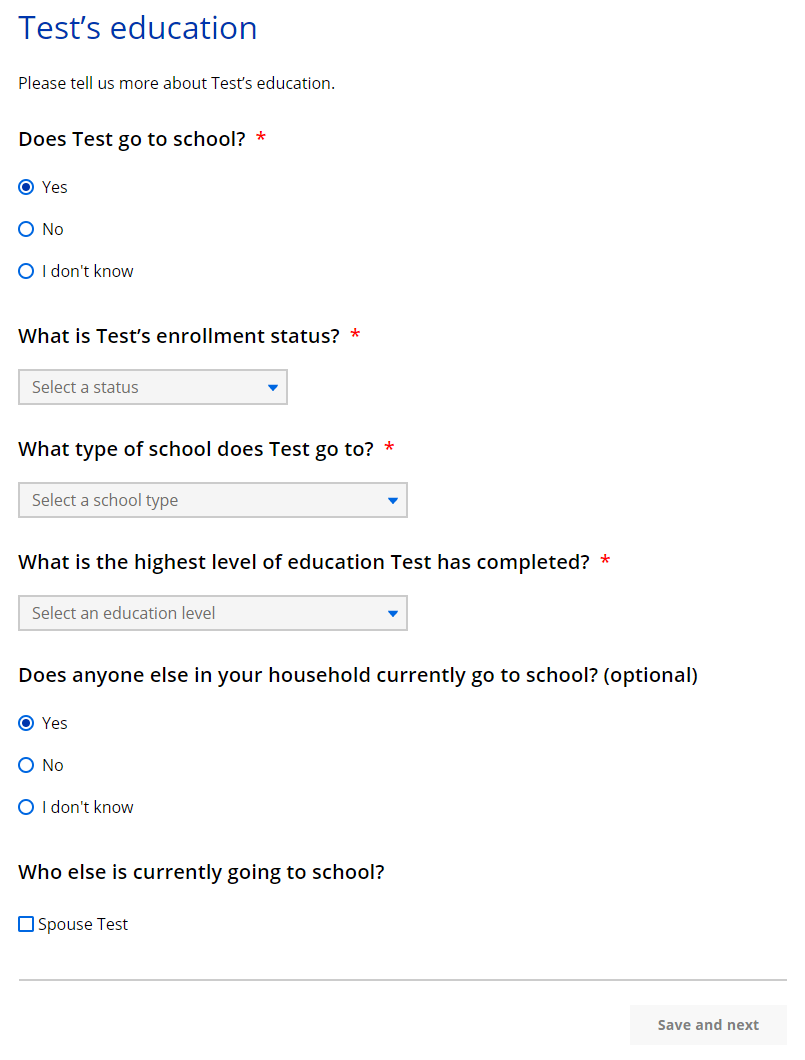
| Questions | How to answer |
| Does _____ go to school? |
Select Yes, No, or I don’t know. |
|
What is _____’s enrollment status?
|
This question is optional for those only applying for Wisconsin Shares Child Care Subsidy. |
|
What type of school does _____ go to?
|
This question is optional for those only applying for Wisconsin Shares Child Care Subsidy. |
|
Do any of these situations apply to ______? (optional)
|
Select which situation or situations apply to the applicant. |
|
When will _____ graduate high school?
|
This question displays if the applicant or household member is attending school (not college or vocational schools). Select the date from the calendar. |
|
What is the highest level of education _____ has completed?
|
Select the highest education level achieved by applicant from the drop-down menu. |
| Does anyone else in your household currently go to school? (optional) |
Select Yes, No, or I don’t know. |
|
Who else is currently going to school?
|
Select which member or members of the household that is currently enrolled in school. The page repeats for the other people selected. |
Step 11: Legal history
This page only displays if the application includes FoodShare, Wisconsin Shares Child Care Subsidy, W-2, or JAL and asks if there are any household members recently convicted of a drug felony, fleeing from a felony, or in violation of probation or parole.
Show/Hide an example of the pageShow/Hide an example of the page

| Questions | How to answer |
| Has anyone in your household been convicted of a drug felony in the last five years? | Select Yes or No. If the applicant selects yes, the next question displays. |
|
Who was convicted of the felony?
|
Select which member or members of the household has been convicted of a drug felony in the past five years. |
| Is anyone in your household fleeing from a felony or in violation of probation or parole? | Select Yes or No. If the applicant selects yes, the next question displays. |
|
Who is fleeing from a felony or in violation of probation or parole?
|
Select which member or members of the household currently fleeing. |
The next page the applicant sees depends on who is in the household and the programs they are applying for.
| If the household includes... | And the application... | Continue to... |
| A Childless Adult | Doesn't include health care | Step 12: Confirm information on the Summary page |
| No Childless Adults | Includes any programs | Step 12: Confirm information on the Summary page |
Step 12: Confirm Information on the Summary Page
Once completed, a summary page displays. Here, the applicant can review the sections for accuracy before going to the next section.
Show/Hide an example of the pageShow/Hide an example of the page

This page last updated in Release Number: 24-03
Release Date: 11/15/2024
Effective Date: 11/15/2024