3.10 Health Insurance
Contents
- Step 1: Answer who currently has a health insurance policy
- Step 2: Provide information on premiums and coverage dates
- Step 3: Provide information on the insurance company
- Step 4: Provide additional information about the household member’s insurance source
- Step 5: Additional health insurance
- Step 6: Answer who has access to health care coverage
- Step 7: Provide information on the source of the available insurance
- Step 8: Confirm information on the Summary page
Use these instructions to help people answer questions about their health insurance. This section is only included if the application includes health care or FoodShare.
A variation of this section is included for Katie Beckett Medicaid applications that only asks questions about the policies for the children requesting Katie Beckett Medicaid.
Once completed, the applicant can review the section for accuracy before going to the next section.
Step 1: Answer who currently has a health insurance policy
These pages ask about the household’s current health insurance. The pages appear for FoodShare applications, Medicaid, FPOS and BadgerCare Plus applications.
The “Health insurance policy holders” page asks if any household members currently have health insurance.
Show/Hide an example of the pageShow/Hide an example of the page

| Questions | How to answer |
| Does anyone have a health insurance policy that covers one or more people in your household? |
Select Yes or No. |
|
Who is the owner of the health insurance policy?
|
Select the owner of the health insurance policy. If someone outside of the household owns the insurance policy, select Someone else. This question is optional for those only applying for FoodShare. |
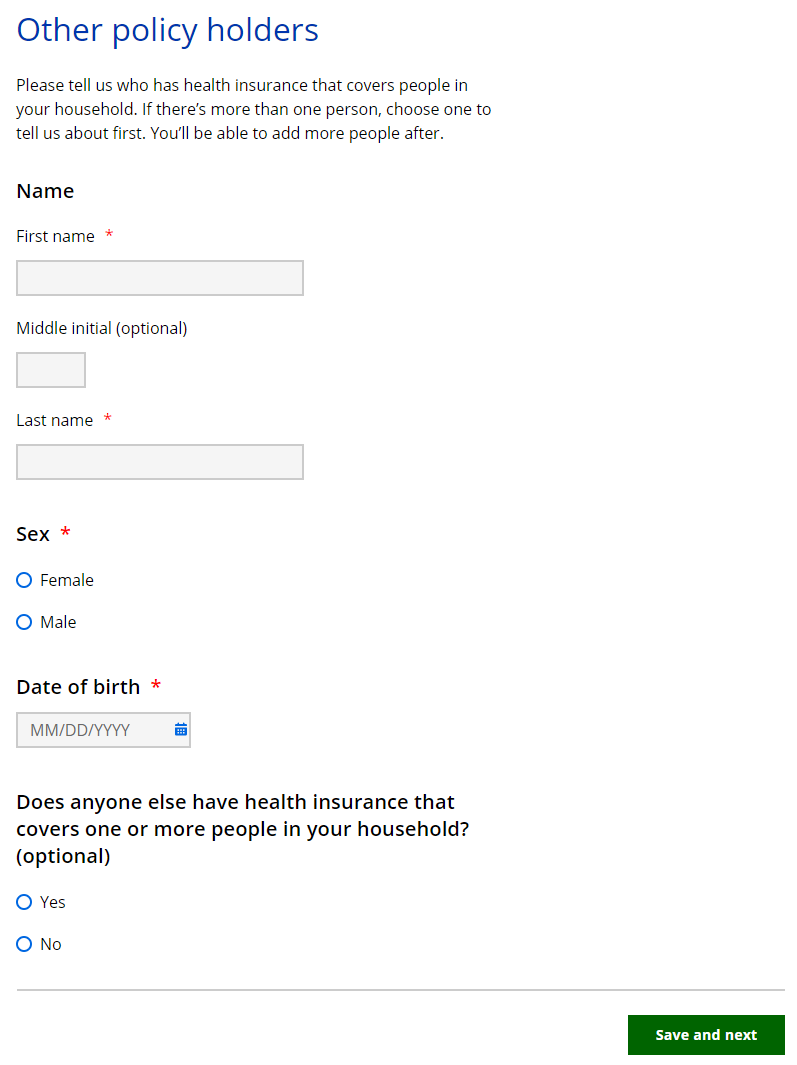
The “Other policy holders” page asks about the individual outside the household who covers people in the household.
Show/Hide an example of the pageShow/Hide an example of the page
| Questions | How to answer |
| Name | Enter the full legal name of the individual. |
| Sex | Select Male or Female. |
| Date of birth | Select the date from the calendar. |
| Does anyone else have health insurance that covers one or more people in your household? (Optional) | Select Yes or No. |
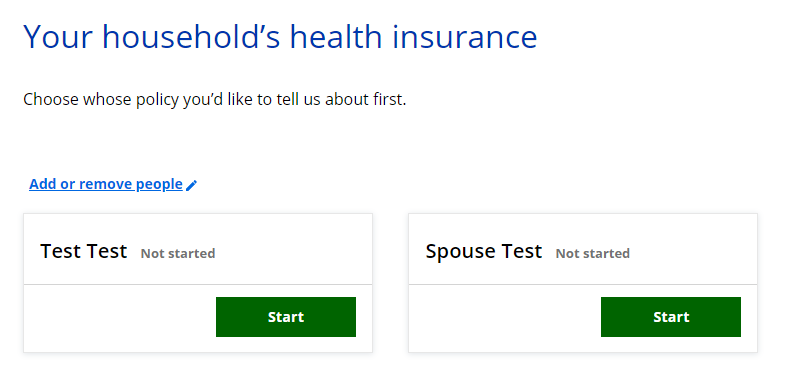
If more than one person in the household has a health insurance policy, the “Your household’s health insurance” page displays. This page asks the applicant to select which household member’s health insurance information to enter first.
The applicant is brought back to this screen until all the individuals who have health insurance are completed.
Show/Hide an example of the pageShow/Hide an example of the page
| Questions | How to answer |
| Choose who you’d like to tell us about first. |
Select Start next to someone’s name to begin asking questions for that person. |
Step 2: Provide information on premiums and coverage dates
These pages ask about the health insurance policy indicated on the previous page. They repeat for each person with a policy.
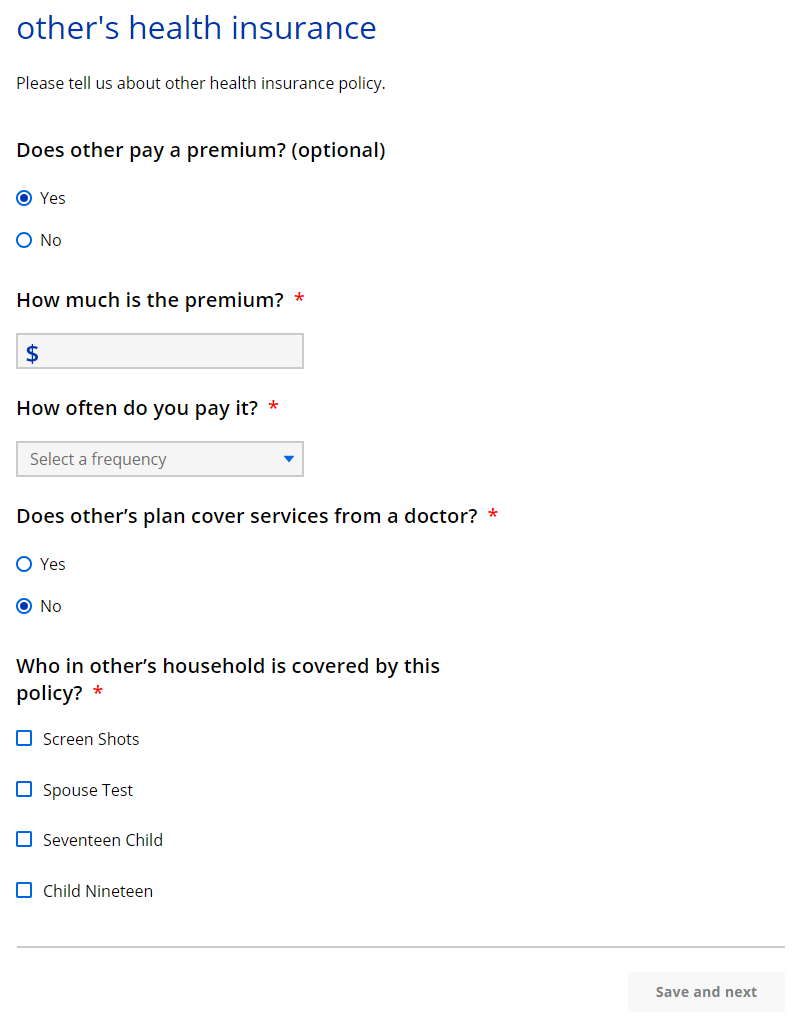
The “_____’s health insurance” page asks about the health insurance policy.
Show/Hide an example of the pageShow/Hide an example of the page
| Questions | How to answer |
| Does _____ pay a premium? (Optional) |
Select Yes or No. |
|
How much is the premium?
|
Enter the premium amount. |
|
How often does _____ pay it?
|
Select the frequency from the dropdown menu. |
| Does _____’s plan cover services from a doctor? | Select Yes or No. |
| Who else in your household is covered by this policy? | Select the member or members covered by this policy. |
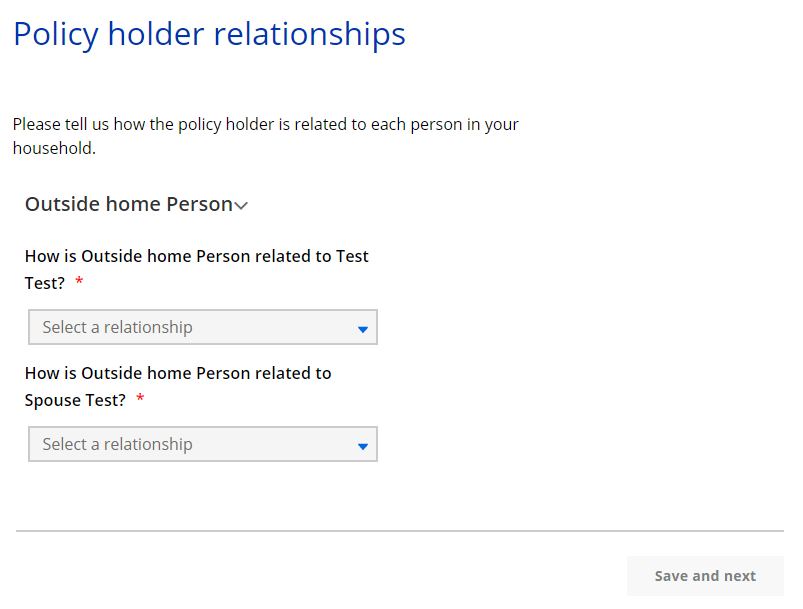
The “Policy holder relationships” page asks about how the policy holder who is outside the home is related to household members.
Show/Hide an example of the pageShow/Hide an example of the page
| Questions | How to answer |
| Relationship to [Household Member Name] | This question repeats for each combination of people in the household. If the relationship has already been described, the answer prepopulates the next time it is asked. |
The “Coverage periods” page asks about the coverage start date for the health care policy.
Show/Hide an example of the pageShow/Hide an example of the page

| Questions | How to answer |
| When did _____’s coverage begin? |
Select the date from the calendar. |
| Will _____’s coverage end in the next 3 months? | Select Yes or No. If the applicant selects yes, the next question displays. |
|
When will _____’s coverage end?
|
Select the date from the calendar. |
The next page the applicant sees depends on the programs they are applying for.
| If the application includes... | Continue to... |
| Health care | Step 3: Provide information on the insurance company |
| FoodShare only | Step 5: Additional health insurance |
Step 3: Provide information on the insurance company
The “_____’s policy information” page asks about the insurance company and plan.
| Questions | How to answer |
| What company offers [Policy holder name's] policy? (Optional) |
Enter the name of the company. |
| Street address | Enter the full address of the company. |
| Health plan name (Optional) | Enter the health plan name. |
| Policy number (Optional) | Enter the policy number. |
| Group number (Optional) | Enter the group number. |
The next page the applicant sees depends on the programs they are applying for.
| If the application... | Continue to... |
| Includes BadgerCare Plus |
Step 4: Provide additional information about the household member’s insurance source |
| Does not include BadgerCare Plus | Step 5: Additional health insurance |
Step 4: Provide additional information about the household member’s insurance source
These pages ask for more information about how the household member has access to insurance, including if they will have continued access into the next year.
The “More about _____’s health insurance” page asks about the source of the health care policy and plan details.
Show/Hide an example of the pageShow/Hide an example of the page
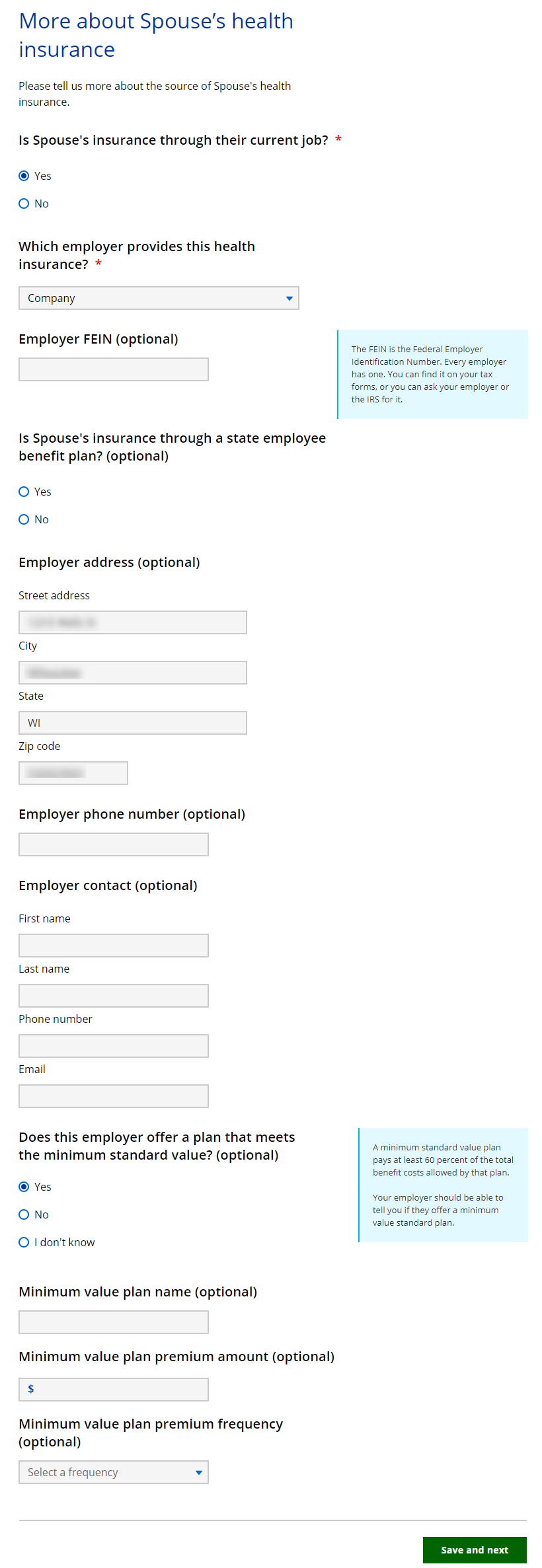
| Questions | How to answer |
| Is _____’s insurance through their current job? |
Select Yes or No. |
|
Where does _____’s insurance come from?
|
Select the source from the dropdown menu. |
|
Which employer provides this health insurance?
|
Select the employer that provides health insurance.
The list shows employers previously entered by the applicant. |
|
Employer FEIN (Optional)
|
Enter the FEIN number of the employer. |
|
Is _____’s insurance through a state employee benefit plan? (Optional)
|
Select Yes or No. |
|
Employer address (Optional)
|
Enter the full address of the employer. |
|
Employer phone number (Optional)
|
Enter the phone number of the employer. |
|
Employer contact (Optional)
|
Enter the contact’s full name, phone number, and email address. |
|
Does this employer offer a plan that meets the minimum standard value? (Optional)
|
Select Yes, No, or I don’t know. |
|
Minimum value plan name (Optional)
|
Enter the name of the plan. |
|
Minimum value plan premium amount (Optional)
|
Enter the premium amount. |
|
Minimum value plan premium frequency (Optional)
|
Select the frequency from the dropdown menu. |
The “Next year’s coverage” page asks about potential changes to the health care policy in the next year.
Show/Hide an example of the pageShow/Hide an example of the page
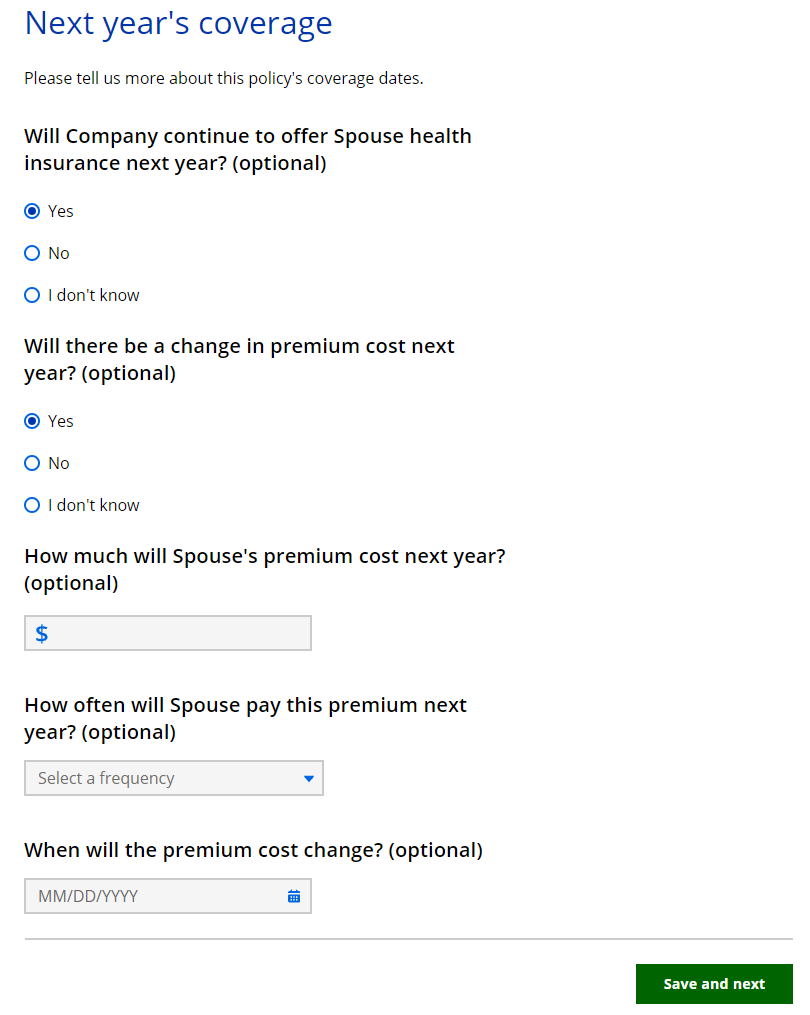
| Questions | How to answer |
| Will [Employer Name] continue to offer [Policy holder name] health insurance next year? (Optional) |
Select Yes, No, or I don’t know. |
|
When will [Policy holder name] lose access to this health insurance? (Optional)
|
Select the date from the calendar. |
| Will there be a change in premium cost next year? (Optional) |
Select Yes, No, or I don’t know. |
|
How much will [Policy holder name’s] premium cost next year? (Optional)
|
Enter the cost of the premium. |
|
How often will [Policy holder name] pay this premium next year? (Optional)
|
Select the frequency from the dropdown menu. |
|
When will the premium cost change? (Optional)
|
Select the date from the calendar. |
The “Can anyone else get coverage?” page asks if anyone in the household could be covered by the health care policy but is currently not.
Show/Hide an example of the pageShow/Hide an example of the page
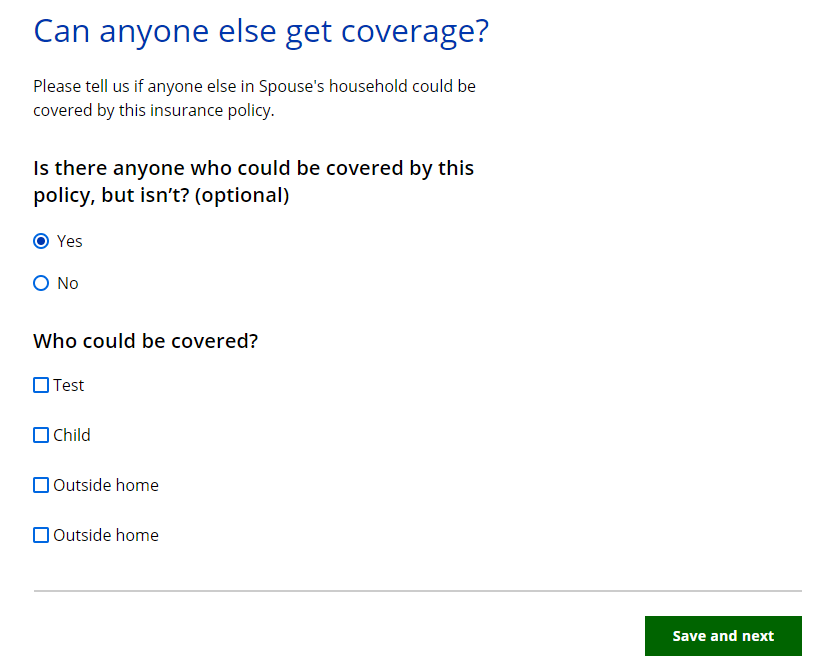
| Questions | How to answer |
| Is there anyone who could be covered by this policy, but isn’t? (Optional) |
Select Yes or No. |
|
Who could be covered?
|
Select the member or members that could be covered. |
Step 5: Additional health insurance
This page asks the applicant if the policy holder has another health care policy.
Show/Hide an example of the pageShow/Hide an example of the page
| Questions | How to answer |
| Does [Policy holder name] have another health insurance policy that covers someone in your household? (Optional) | Select Yes, No, or I don’t know. |
The next page the applicant sees depends on the programs they are applying for.
| If the application... | Continue to... |
| Includes BadgerCare Plus |
Step 6: Answer who has access to health care coverage |
| Does not include BadgerCare Plus | Step 8: Confirm information on the Summary page |
Step 6: Answer who has access to health care coverage
The “Additional access to coverage” page asks who in the household has access to health care but is not currently enrolled.
Show/Hide an example of the pageShow/Hide an example of the page
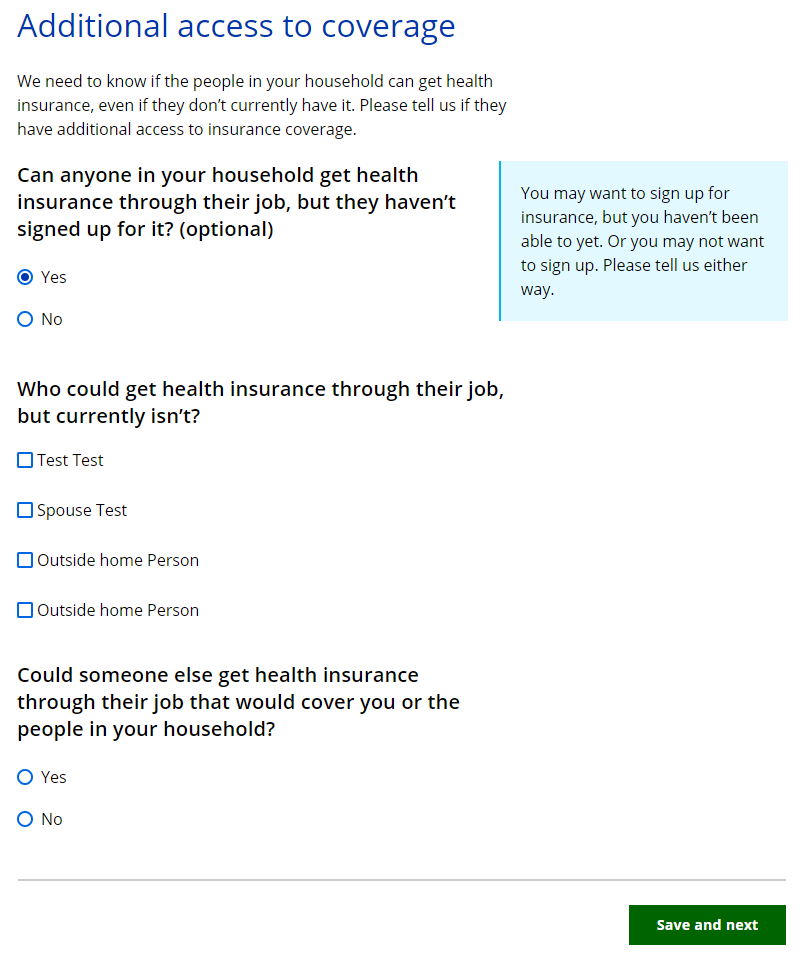
| Questions | How to answer |
| Can anyone in your household get health insurance through their job, but they haven’t signed up for it? (Optional) |
Select Yes or No. |
|
Who could get health insurance through their job, but currently isn’t?
|
Select the member or members that can get health insurance through their job but currently does not. |
|
Could someone else get health insurance through their job that would cover you or the people in your household?
|
Select Yes or No. |
The “People who could get insurance” page asks about how the policy holder who is outside the home is related to household members.
Show/Hide an example of the pageShow/Hide an example of the page
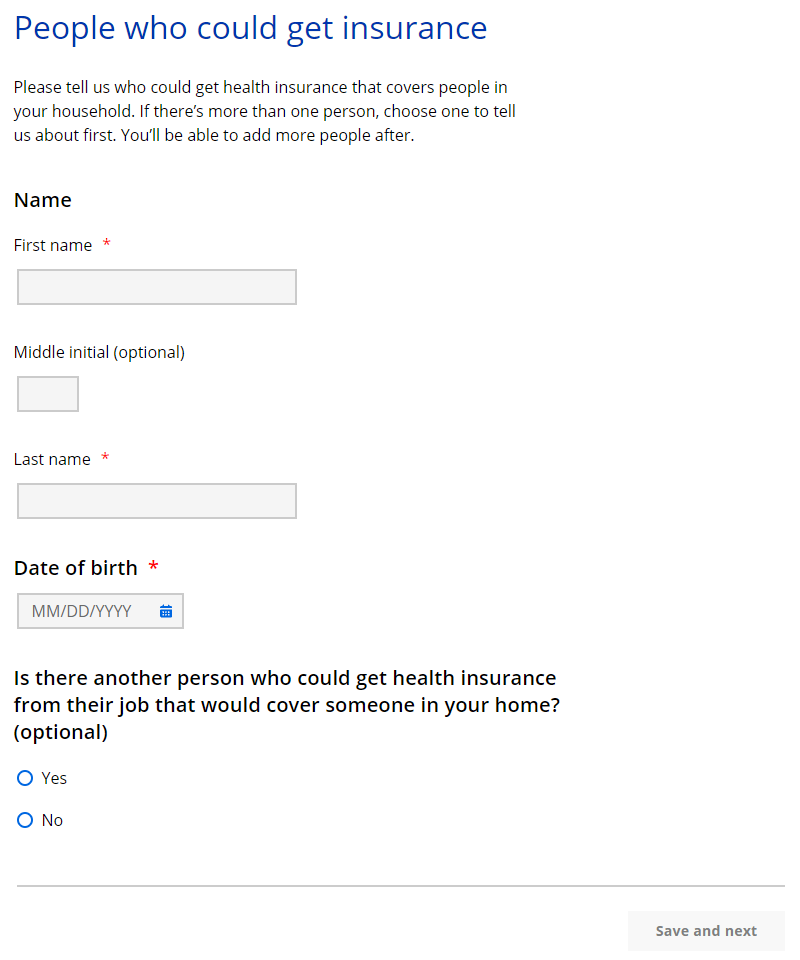
| Questions | How to answer |
| Name | Enter the full legal name of the individual who can cover people in the household. |
| Date of birth | Select the date from the calendar. |
| Is there another person who could get health insurance from their job that would cover someone in your home? (Optional) | Select Yes or No. |
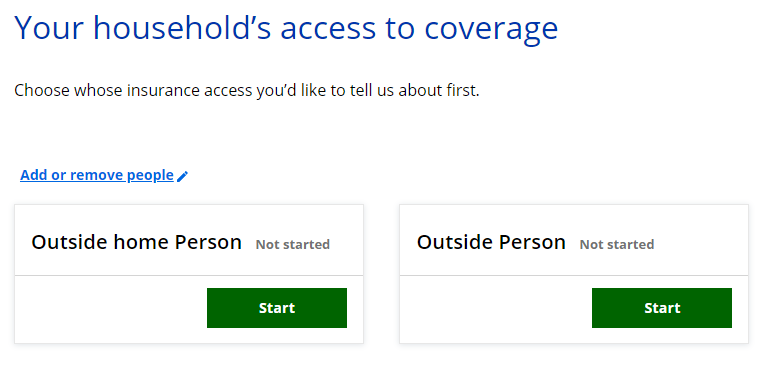
If more than one person in the household has a health insurance policy, the “Your household’s access to coverage” page displays. This page asks the applicant to select which household member’s health insurance information to enter first. The applicant is brought back to this screen until all the individuals who have health insurance are completed.
Show/Hide an example of the pageShow/Hide an example of the page
| Questions | How to answer |
| Choose who you’d like to tell us about first. |
Select Start next to someone’s name to begin asking questions for that person. The applicant is brought back to this screen until all the questions for individuals who have health insurance are completed. |
Step 7: Provide information on the source of the available insurance
These pages ask for more information about how the household member has access to insurance, including if they will have continued access into the next year.
The “_____’s job that offers coverage” page asks about the source of the health care policy and plan details.
| Questions | How to answer |
| Which employer provides this health insurance? |
Select the employer that provides health insurance. |
| Employer FEIN (Optional) | Enter the FEIN number of the employer. |
| Is this insurance offered through a state employee benefit plan? (Optional) | Select Yes or No. |
| Employer address (Optional) | Enter the full address of the employer. |
| Employer phone number (Optional) | Enter the phone number of the employer. |
| Employer contact (Optional) | Enter the contact’s full name, phone number, and email address. |
| Does this employer offer a plan that meets the minimum standard value? (Optional) |
Select Yes, No, or I don’t know. |
|
Minimum value plan name (Optional)
|
Enter the name of the plan. |
|
Minimum value plan premium amount (Optional)
|
Enter the premium amount. |
|
Minimum value plan premium frequency (Optional)
|
Select the frequency from the dropdown menu. |
The “Next year’s access to coverage” page asks about potential changes to the household member’s health care coverage in the next year.
Show/Hide an example of the pageShow/Hide an example of the page
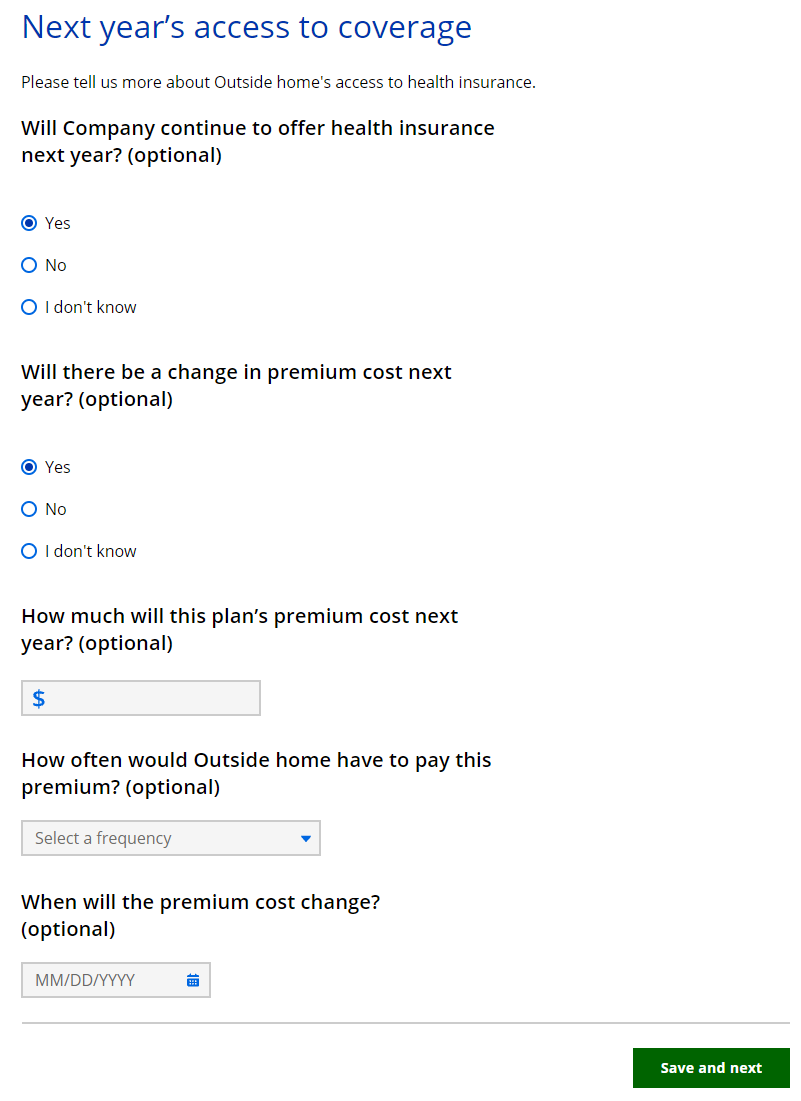
| Questions | How to answer |
| Will [Employer Name] continue to offer health insurance next year? (Optional) |
Select Yes, No, or I don’t know. |
|
When will [Policy holder name] lose access to this health insurance? (Optional)
|
Select the date from the calendar. |
| Will there be a change in premium cost next year? (Optional) |
This question displays if the applicant selects yes on the first question. |
|
How much will this plan’s premium cost next year? (Optional)
|
Enter the cost of the plan for the next year. |
|
How often would _____ have to pay this premium? (Optional)
|
Select the frequency of the payment from the dropdown menu. |
|
When will the premium cost change? (Optional)
|
Select the date from the calendar. |
The “Could anyone else get coverage?” page asks who in the home could be covered by the health insurance plan offered by this individual’s employer.
Show/Hide an example of the pageShow/Hide an example of the page
| Questions | How to answer |
| Is there anyone who could be covered by this policy, but isn’t? (Optional) |
Select Yes or No. |
|
Who could be covered?
|
Select the member or members who could be covered. |
The “Is _____ waiting to enroll?” page asks if the individual plans to enroll in this health insurance plan or is in a waiting or probationary period.
| Questions | How to answer |
| Is _____ in a waiting or probationary period? |
Select Yes, No, or I don’t know. |
|
When will the probationary period end?
|
Select the date from the calendar. |
| Does _____ plan to sign up for this health insurance in the next three months? |
Select Yes, No, or I don’t know. |
|
When does _____ plan to enroll?
|
Select the date from the calendar. |
The “Additional health insurance” page asks if the household member has another health insurance policy through an employer that they could be on.
Show/Hide an example of the pageShow/Hide an example of the page
| Questions | How to answer |
| Does [Policy holder name] have access to another health insurance policy that covers someone in your household? (Optional) | Select Yes, No, or I don’t know. |
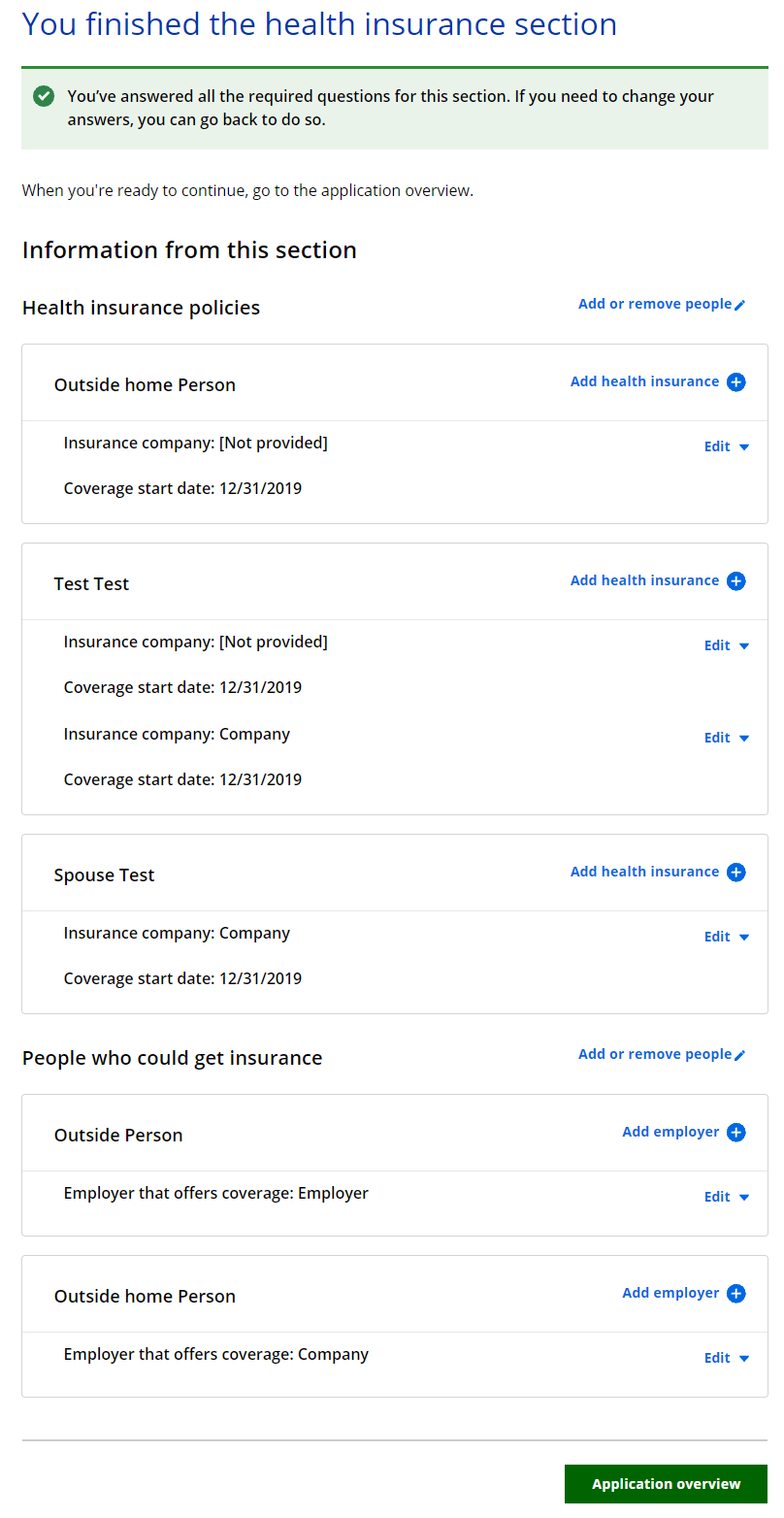
Step 8: Confirm information on the Summary page
Once completed, a summary page displays. Here, the applicant can review the sections for accuracy before going to the next section.
Show/Hide an example of the pageShow/Hide an example of the page
This page last updated in Release Number: 24-03
Release Date: 11/15/2024
Effective Date: 11/15/2024